Pat McGuigan, Smash Up The Workhouse Smash up Workfare
Noel Smith, Star of David
Aaron WJ Pilgrim, Michael Drawing Futuristic Cars
Sarah Davies, Leicester Square Busker
Liz Innes, Lake district landscape
Sarah Davies, Black and White Man Dr Salter
William Ball, Face to Face
Ese Imonioro, Gotcha
Aaron WJ Pilgrim, Grace
Graeme Newton, Help
Hope is the focus of a new exhibition by artists from the CoolTan arts and mental health charity.
Stayin’ Alive, which opens today, includes works in different media including oil on canvas, acrylic, printmaking and sculpture. The stigma-breaking south London-based organisation is run by and for people with mental health issues and encourages the idea that mental wellbeing is inspired by creativity. The recent World Mental Health Day was the impetus for the artworks.
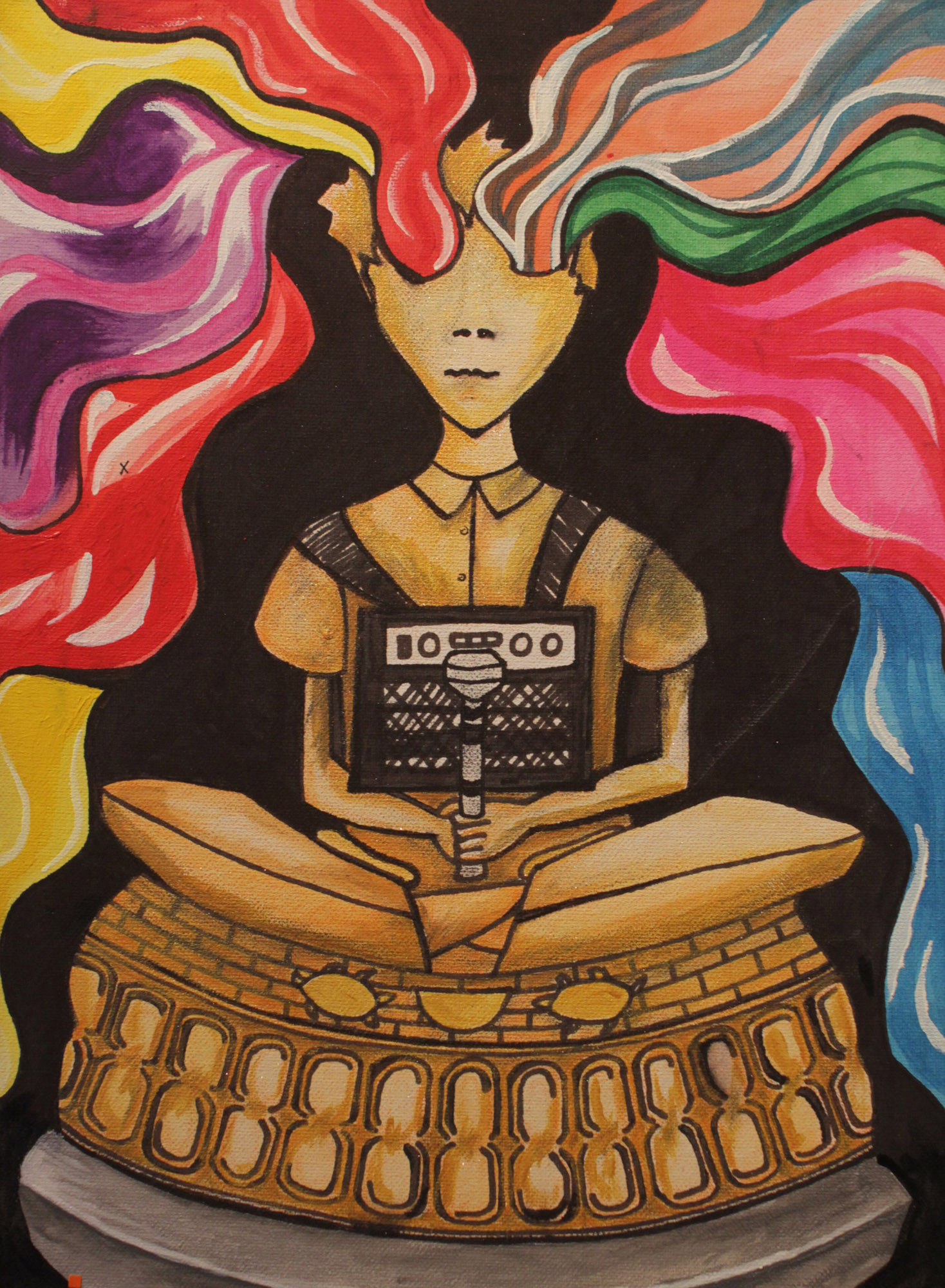
Aaron Pilgrim has four pictures in the exhibition and has been involved in CoolTan for five years. His Warhol-like Music (Martika) (above) is about the impact of music on mental health (“and I love listening to the 80’s pop star Martika”). Aaron’s last picture, Drawing futureristic cars (Michael), reflects how he helped to frame the exhibition and taught two volunteers how to mount, cut and frame pictures in the exhibition.
He says of The Globe Theatre & The Tate Modern “the arts help keep me well, especially painting, and these two places represent the arts. This picture is in the style of Turner.
Another of Aaron’s picture, My beautiful daughter Grace is about “being a good dad & my family help keep me well”.
Liz Innes, who has been attending art classes at CoolTan for around seven years, shows piece depicting a Lake District landscape. Liz adds: “I wanted to submit my landscape painting which was inspired by a photograph I took 20 years ago. I enjoyed painting this as it reminds me of my younger, more lively days when I often went walking with friends. I have really enjoyed my work in pen and ink recently and feel it is developing well. I have received a lot of encouragement from the staff and tutors at CoolTan.”
Marjorie Mclean, who has been involved with CoolTan for eight years, is showing her watercolour My Allotment. “For me going to the allotment, being in the sunshine and seeing things grow, producing food, makes me feel hopeful and happy”, she says.
Marjorie McLean, My AllotmentEse Imonioro, Gotcha
Ese Imonioro’s work in collage and felt-tip was done about a difficult time in her life” “At that moment I felt quite persecuted, but I could not convince anyone of what was happening. The painting is of a doctor who helped me during this period and made everyone see the truth. I will always be eternally grateful to him for that and for giving me my freedom.”
Lynn Hughes, Kingfisher
* The CoolTan exhibition runs until 26th November, Monday to Thursday 10-5:45, Fridays 10-5 at CoolTan Arts, third Floor, 224-236 Walworth Road, SE17 1JE
Bullying crushes a child’s self esteem and confidence. It can leave a child feeling alone, totally helpless, and with no one to turn to. In their childhood innocence and naivety some even blame themselves for their torment. Many schools now have robust anti bullying policies in the form of bullying charters.
We live in an age where teachers acknowledge widely the emotional needs of children more than ever before. Resources such as SEAL (social and emotional aspects of learning) provide increased emotional support in many schools.
As a consequence bullying has now left many classrooms, but not all. This is commendable but, not only do schools’ attitudes and actions in response to bullying vary considerably, is it enough?
And now in the age social networking sites it has insidiously entered the sanctuary of children’s bedrooms. Running away from the school environment and threatening bullies now leads straight to the bedroom, a once safe haven where a child’s computer suddenly provides no way of escape. Computers are the contemporary child’s toy and some may say the innocence of youth has died as a result. This year’s forthcoming Anti-bullying Week, for example, has a special focus on cyber-bullying.
These issues have been on my mind since the death of 14-year-old Hannah Smith who suffered relentless bullying online. Her death was not a stark reminder of how vulnerable our children are not protected from bullies even in the supposed safety of their own homes. There has been intense speculation and much knee-jerking as a result of her death, but the bottom line is that social media played a part in her suicide. Whatever happened, she was a vulnerable child.
But social networking sites can be so liberating for many providing an outlet for those who lack self confidence in face to face interactions and who might have smaller social networks than usual. Many can make friends and form relationships online that they would otherwise struggle to in school.
These sites can be very helpful, especially for those who lack social contact, or may have poor social skills, agoraphobia etc, but the flip side of the coin is the bullying issue. Reaching an acceptable compromise regarding social networking will not be easy because the genie has now been let out of the box, so to speak.
When experiencing low moods, your reality becomes alien to that of everyone else. I have always advised people to seek help at the earliest opportunity to prevent depression reaching this critical stage. And this is where social sites that support mental health can help.
There is the social site launched by comedian Ruby Wax, for example, Black Dog Tribe, “a place in which like-minded people can find their own ‘tribe’ and share experiences in a supportive online community through forums, blogs, daily news and mental health information”. Another example is Kent and Medway NHS Trust, for example, which is piloting Buddy, an online system that records mood changes. And there are a raft of support-specific online forums linked to various charities and support groups which can make all the difference to vulnerable people.
This is the positive aspect of these sites.
Yet it is too simplistic an argument that social media and networks alone can help prevent depression. An holistic approach can include talking therapies, physical exercise and medication, if appropriate. These therapies can support each other – medication, as I know from personal experience and from my nursing career, has its down side. It can also make your mood fluctuate wildly, become disinhibited and even suicidal. Having easy access to online support can, at times like this, be vital. These issues are brought into sharp focus by the news today that the number of people needing treatment for mental health issues will have increased by more than 2 million by 2030.
We should look closely at both the negatives and positives about social media and networks in relation to mental health – and ignore them at our peril. While it is also wrong to assume that social media alone can push someone towards mental health problems, excessive use of social sites, as is often reported, can itself lead to problems.
Children sitting for hours in front of a screen removes them from the social contact of others that will improve their face to face communication skills and confidence in later life. Effective communication involves eye contact, body language, and gesturing. All ignored when lying in bed hitting a keyboard in silent and lonely surroundings.
Cyber bullies and unpoliced social media sites populated by children (or those posing as children) are not part of a civilised society. We must make it all stop. Now.
Helen Knowles, “Birth with Orgasm” (image courtesy of the artist and GV Art gallery)
Hyper-real images that question cultural attitudes towards women and childbirth form part of a new exhibition opening today.
The show at the GV Art gallery by Helen Knowles, Private View: Public Birth, features both figurative and abstract images of women “in the transcendental state of birth”; Knowles founded the Birth Rites Collection in 2008, the first collection of contemporary art dedicated to the subject.
Knowles has used screen grabs from YouTube videos to show women at the crowning stage of birth, when the baby’s head beings to emerge. By using footage from social media platforms – films usually reserved for private viewing – Knowles hopes to question the discomfort some audiences have with certain images.
The Birthing of Azheyo Aeoro (Image courtesy of artist and GV Art)
The concept is a refreshing and thought-provoking one. Most public perceptions of new mothers involve images of immaculately groomed famous women whose bodies magically snap back into place and while “beautiful” is a word often used to describe babies, it’s rarely associated with birth itself (and certainly not linked to images of the birth process).
Yet the pieces of work on display in today’s exhibition are intriguing and often ethereal, reflecting notions of female strength.
* Private View: Public Birth, a curatorial collaboration between Poppy Bowers and Helen Knowles, runs from 16-22 September at the GV Art gallery, Marylebone, London.
Building relationships with children at risk of care helps keep them at home (pic Includem/Warren Media).
The fate of children in care in Scotland has recently his the headlines; care leavers need more support, say experts, if their life chances are to improve. And today Michael Gove has criticised the care home system in England. But what if some vulnerable children could be prevented from going into care in the first place? In a joint guest post, Daniel* and the support worker who helped him describe how a Scottish community-based alternative to custody and secure care helped him turn his life around.
Daniel*, 21, describes how he was supported by the charity Includem:
“I don’t even know if I would be alive had it not been for Includem. I was drinking all the time and taking drugs, valium, cannabis, ecstasy. I was fighting a lot with my mum and other people and ‘doing turns’ – theft, breaking and entering offences – to get money to spend on food and clothes. Things started to go wrong when I left primary school and when I was about 12.
I had a bad relationship with my mum – we argued all the time – and I was constantly getting thrown out of the house. I had nowhere to go so ended up on the streets. I was always in front of children’s panels and going into temporary care and then home again.
I wasn’t happy and could see that this [drinking and taking drugs] wasn’t the right thing to do but it was what was happening in my life at the time. I felt guilty about what I was doing. I wanted things to change but didn’t now how to make changes. I wanted things to be normal and to have a normal family life.
A social worker referred me to Includem; I worked with a few project workers until I clicked with my project worker who became the person who I felt I could work with. We spoke about goals and how to get there and how I was worthy of a better life.
My worker helped me when things were really bad at home; I could call the helpline at any time and Includem would come out and talk to me and my mum and make it ok for me to stay at home. They would meet with me at times when no one else would be able to – at the weekend, when I needed them I would contact the helpline and they would be there.
Includem helped me stay at home and they helped me get into training and never gave up on me. I respected them and they respected me. I felt hopeful that things could be different. They helped with all sorts of things – planning how to spend money on food and clothes to helping with how to deal with bad situations at home and how to get training to help to get a job.
They were there through everything – even during the night – when I lived at home, when I was homeless and then moving into my own place. They made me think that I was worthwhile.
Before I would just go out and steal things to sell so that I could buy new clothes. I learnt how to save money and how to spend it on food so that I would last. They taught me how to deal with situations with my mum – how to walk away from violent situations and how to stay calm.
Things changed for me because my worker listened and respected me so I trusted and listened to my worker. I got on with her and established a relationship – I started to feel hopeful that things could change. Includem listened and didn’t give up on me, even at the start when I didn’t want to work with them.
Now I live with my daughter and girlfriend and I have my own home. I try hard to be a good dad that my daughter can be proud of – I want her to feel loved and cared for and safe. I want a routine for my family and my daughter and I am trying to find a job.”
Karen McCulloch, Includem project worker, on how she supported Daniel:
“Daniel was referred to Includem at the age of 15 due to his drug and alcohol misuse, anger, aggression, and difficult family relationships. He was a persistent high tariff offender and was facing homelessness due to a chaotic relationship with his mother.
When we meet a young person for the first time we listen to what they have to say and let them know what we can offer. We talk through their lives and identify the areas that aren’t working the way they should and start to look at how these could get better. We identity goals and talk to them about A Better Life – a unique toolkit that we use. We let them know we will meet them on a frequent basis and that we will plan normal social activities where we can meet and talk.
We let them know we put them first and they can trust us – that we want the best for them. Often this is a first for young people who haven’t had proper care in their lives or someone to talk to and look out for them.
We gave Daniel intensive support in managing his anger, including practical support on issues such as how to remove himself from volatile situations. Daniel’s relationship with his mother was difficult, and Includem worked with her to set clear and consistent boundaries within the home.
Daniel and his mother used Includem’s 24 hour helpline, not only at times of crisis but for advice and support. Includem supported Daniel for whilst he was on an electronic tag, a period in secure care for his own safety, and voluntary transitional support into adulthood. Throughout this time, Includem supported and liaised with Daniel’s mother to maintain their relationship.
Daniel didn’t gel with his first project worker so we changed workers to someone that Daniel clicked with. Our model is relationship based therefore we are flexible and will try different workers with different young people for the right relationship to be established.
My first visit to meet Daniel was on a Friday night when Daniel was out with his care home – Daniel had none of his own clothes so I went to his home and picked these up and took them to him. We visited him throughout the weekend and supported him. We talked about ways to change things – and assured Daniel that his life could change with the right support and direction. We put a plan in place that we would work through together in order to meet outcomes.
We started to see real changes. We taught Daniel to listen to his “inner speak” – the voice within that said he deserved a better life and that he could make it happen. When he started to realise that he did deserve better, and how to achieve it, things started to change.
Daniel used the 24/7 helpline regularly as a support – he would phone if he had been thrown out of the house or was in trouble. He would call if he was arguing with his mother – on one occasion an Includem worker would be speaking to Daniel on the phone in one room, another would be speaking to his mother on the phone in another room and a worker would be driving to the house to help calm the situation face to face.
Daniel would forget basic things such as when to eat as sometimes he was living between people’s houses – we would remind him that this was essential and give him practical support on what to eat and how to budget his money. We would plan our contact visits with him around when he would receive money and would take him to the supermarket and show him how to spend the money wisely and make it last.
Daniel moved into his own home under a mainstream tenancy at 19 (he is now 21), and is in a settled relationship and doing well. He has created his own family – he and his girlfriend have a baby, and there is no social work involvement with the family at all. Daniel has accrued no court charges or pending court charges for fouryears. He’s very keen to get a job. His partner is looking to start college and his main aim is to build on his progress and continue to provide a happy and loving environment for his child and partner.
We have a “scaffold of support” in place – a team of three – a project worker, an assistant project worker and a mentor – assigned to each young person so that they can build links and relationships with more than one person. Every service we provide is unique for that young person – we fit our service to them, not the other way round.
Among our successful outcomes is the fact that 90% of young people we worked with in a project with Strathclyde police reduced their violent offending. And with 72% of referrals from the Clackmannanshire area, Includem prevented family or community placement breakdown.
The biggest challenge is usually at the outset when young people are wary of accepting help and opening up about issues. Another challenge is actually meeting up with young people on planned visits at the start– often they don’t turn up for planned meetings and we have to go looking for them.
You learn to be creative in situations like this – finding solutions to challenges such as this and others – and speaking to colleagues for advice and ideas in order to make contact. We constantly refer to our A Better Life toolkit for support and advice.
Includem operates 24 hours a day, 365 days a year. We accept any referrals via social work departments, courts and police. We never turn any vulnerable young person away – no matter what their situation is and how chaotic it may be.
‘Stickability’ is a word we have coined – it’s a key part of our service and is at the heart of what we do – we are persistent, we won’t give up on a young person and we will stick with them at all times during the support we give them.”
Society often fails to realise that people aged 65 and over currently represent a sixth of the UK population responsible for £120 billion worth of spending power a year – over 18% of total spending in the UK. And the number of people aged 65 and over is projected to rise by nearly 50% in the next 20 years to over 16 million (figures from the Office for National Statistics).
As Britain adapts to an ageing population, the marketplace for assisted living aids and adaptions such as stairlifts, adapted bathrooms, wheelchairs, mobility scooters and pendant alarms will become a dominant area of spending. Market forces will encourage producers and distributors to sharpen up their communications to older people but it would be a very positive development if we were to address this now rather than later.
The government’s 3 million lives initiative, announced last year with the aim of improving access to telecare and telehealth, is an important step towards transforming service delivery for people with long term conditions, and/or social care needs, by utilising telehealth and telecare within health and social care services. Telecare and telehealth relate to the use of technology-related devices, from high-tech equipment to simple sensors, that help people maintain their independence and boost their safety. And during a recent debate on the Care Bill in the House of Lords the government announced that it intends to maintain existing entitlements for older people regarding aids, minor adaptations and intermediate care.
These developments are warmly welcomed. However recent research by Age UK Enterprises, the commercial arm of the charity, found that there is still a way to go in ensuring that knowledge about these developments is passed to those who most need them. The survey revealed that 20% of over 65s feel there is a lack of information available about independence aids for the home.
The low consumer awareness amongst people aged 50-70 of the very products which can aid independent living at an older age can be addressed. But there are also social perceptions that we need to tackle too. A key finding from the research conducted by the Health Design & Technology Institute (HDTI) at Coventry University in partnership with Age UK and campaigning charity Grandparents Plus, is that while some in later life would benefit from independence aids, many older people do not want to be stigmatised or singled out as being in need of “assisted” products or “equipment”.
Age UK Enterprises is interested in this as we provide personal alarms (one of many aids that help older people remain independent within their own home). It is imperative that the utmost is done to prevent falls and accidents within the home and these aids are a step in the right direction to ensure the protection of this demographic (NHS figures show that around 30% of adults over 65 and living at home will experience at least one fall a year and this rises to 50% of adults over 80 who are at home or in care).
So we need to collectively tackle these issues by thinking comprehensively. From their inception and design these products need to help avoid stigmatising older people by ensuring good, attractive, non-medical design. Their availability needs to be considered too.
Out Age UK Engage Business Network aims to share knowledge and insight about what the ageing process means for business best practice. It encourages better design of mainstream products and services to meet the needs of our ageing populationThe Network is seeing more and more businesses waking up to the idea of making services and products easier to engage with and inclusive; not just subsets of their product range aimed at the older market but their entire offering. If done well, this will naturally make brands accessible to all customers, including people in later life.
We must help older people realise how much support is available to them. There are solutions available to help improve their independence, as well as their confidence in the support available to them. This support network is substantial and includes everyone from charities and businesses, through to local authorities and the government, and each element has its part to play in raising awareness of independence aids.
* Gordon Morris is managing director of Age UK Enterprises. Age UK’s ‘Adapting your home’ guide includes information about the aids that can enable older people to stay independent in their own homes for longer; for a free copy call Age UK Advice free on 0800 169 6565 or visit www.ageuk.org.uk to download a copy.
A resident of Hinnerup Kollegiet, a Danish community of older people with autism (pic: Hinnerup Kollegiet)
Timothy Baron was among the first children in the UK to be diagnosed with autism just over 50 years ago. Timothy was in need of specialist education but autistic children then had no right to schooling, so his father, Michael, opened his own school, the movement became the Society for Autistic Children – now the National Autistic Society (NAS).
That was the 1960s; today, Timothy, who lives in residential care, is nearing 60. The first generation of children to be diagnosed with autism is now moving into older age. Ageing with autism brings not only the particular challenges of the condition – communication, social interaction or sensory issues – but the social, physical and mental health issues often experienced in old age.
Policymakers are aware of the impact on society of the ageing population, but the same focus has not been given to people with learning disabilities and autism.
Read the rest of my piece about the need for more work on autism and growing older in the Guardian’s social care pages.
Stephen Fry’s recent disclosure of his attempted suicide last year highlights that mental illness does not discriminate between the “haves” and “have nots”, the famous and the “ordinary”. None of us are immune from the feelings Fry described.
The representation of mental illness in the media in recent years (you need only think of Frank Bruno’s treatment by the tabloids), in television dramas and soaps has not, over many years been empathic. People with mental health issues seem to be either suicidal or mostly violent and dangerous – the two extremes of mental health geared more towards boosting viewing figures than portraying realism and authenticity.
These exaggerated displays of mental health only perpetuate the stigma and stereotypes. In fact it would be fair to say media representation has often been ignorant, discriminatory, and at times criminalising towards the mentally ill. In fact earlier this month, the actress Glenn Close apologized for her depiction of a mentally ill woman in Fatal Attraction.
Sensationalistic storylines and stigmatising stereotyping have only served to misinform and cloud the viewers image of someone who is ill and needing help – but that someone could be any one of us at any time of our lives.
The Time To Change media advisory service, which I am involved in, was set up to change negative perceptions and offer advice and guidance to promote more realism and sensitivity when covering mental health storylines. Advising the soap Emmerdale on a storyline featuring Zak Dingle, the popular loveable rogue, felt like living a double life for a year as the programme documented how his mental ill health spiraled downwards. Emmerdale provided me with a unique test: to positively influence a popular soap storyline. It afforded me the opportunity to use my own personal experience of depression, and lifetime working as a qualified mental nurse, to bring realism and authenticity for a change. I took on the role with a gusto I had not felt for many years.
I immersed myself in the role to the point of drowning. I knew that only by doing this could I truly empathise with Zak’s plight and engage the viewing public. I read countless scripts going over each one with a fine toothcomb burning the midnight oil. I spoke for hours on the telephone with Fiona, the researcher, and my mobile phone was constantly in use for texting and talking over the scenes. I so wanted this to be right.
I felt duty bound to make a difference having been given this opportunity. I advised that showing Zak’s vulnerability and fragile emotional state, rather then the often stigmatising “Mad axeman is dangerous” image, would encourage the viewer to also empathise more. This worked well and delivered the right message to the viewers.
I was made redundant halfway through this work and understandably my self-confidence and esteem was badly dented. In fact it became non-existent. Conversely my work with Emmerdale helped me regain this. I felt I could empathise more with the Zak character as my mood plummeted. I became Zak, or at least this was how I felt at the time. We walked the same troubled path for a while.
The advisory service will continue to influence and craft storylines around mental health. We will continue to provide personal advice and information to researchers, directors, journalists and the stars themselves to make mental health depictions credible. We will provide guidelines and key tips such as to try to allow the characters storylines time to develop. And that recovery can be a long process.
We will encourage the listening of peoples personal stories, and encourage careful thinking about how the other characters in the soap will react. The use of humour is not necessarily a bad thing and bringing in some humour and warmth will challenge peoples often misinformed stereotypes of mental health.
Mental illness doesn’t make people bad so by reinforcing this we can discourage programmes using a mental health storyline to try and explain bad or strange behaviour. For far too long criminalisation of the mentally ill has existed on TV and Radio and this misperception must change.
We have a long road to walk in our media advisory work to get this right. Or as near to accurate as we can. It is crucial that we walk this long and no doubt winding road together. Through collaboration and mutual respect we will make damaging stereotyping of mental illness a distant memory in the media. It is a win-win situation for all concerned.
* Read more thoughts from Lol on the Emmerdale storyline here
* Tips for storylines featuring mental health issues that create dramatic and interesting narratives without alienating audiences, resorting to stereotypes or using a mental illness to try and explain “bad behaviour”:
– to make a charactor plausible and accurate, speak to as many people who have mental health problems as possible. They are the best consultants available and most want to see accuracy on screen
– think about your camera shots. Certain mental health conditions can lead people to feel isolated or to experience altered reality. This can be reflected through close up shots, POV shots or hand held
– give the storyline enough time to develop. It is common that symptoms of mental health problems will manifest over a period of time and build in intensity, rather than develop and explode in the space of one episode
– think about how other characters react. Stigma and discrimination can be as bad as the mental health problem itself for many people. Can you show any empathy from others?
– get expert advice from mental health charities and experts to ensure that the symptoms you are showing on screen are relevant and realistic
– think of your dramatic climax carefully. Most people with mental health problems are not violent so it is unrealistic for a storyline to always end in violence or homicide
Based on information from the Time to Change media advisory service. Read more here.
“Disabled people in residential care who want to live more independently are being prevented from doing so by funding wrangles between local authorities” – that’s taken from a piece I wrote three years ago, but since then little has changed.
“Caught in a trap: disabled people can’t move out of care”, The Guardian October 2010
Here’s the mess: an individual’s “ordinary residence” is usually in his or her original local authority area, so if a council places someone in residential care outside the area, it remains financially responsible.
But when someone decides to move from that residential care in the new area into supported accommodation within the same (ie “new”) area, their original authority argues that it is no longer responsible for funding. However, the new authority – where the person actually lives – argues against funding someone not originally from the area. The result – limbo.
Confusing? Not really, what it boils down to is that councils are passing the buck over people’s care, effectively dictating where people should live -and all the while, individuals themselves appear to have no say. And quibbling over the care bill will only get worse as local authority cuts continue to bite.
I’ve been involved in a piece of work published today by social care organisation Voluntary Organisations Disability Group. The VODG has previously demanded action to resolve such ordinary residence dilemmas and, this time, it argues that the Care Bill offers ample opportunity to finally tackle the challenge. The new briefing, Ordinary residence, extraordinary mess, is available from the VODG website, with this post outlining how the situation has become “business as usual” in many areas.
One way forward, which the bill could accommodate, is strengthening the duty on local authorities to cooperate with providers and with each other to prevent delays in funding when people want to move from one care setting to another. The Epilepsy Society, for example, which contributed to today’s publication, estimates that in the last three years it has covered gaps in fees totalling £350,000 and “staff time involved in chasing fees over the same period has amounted to approximate 340 days across all departments including senior and service managers, finance and administrative staff”.
Here’s just one story from today’s publication, from a social care provider in central England: “Joe moved out of residential care into supported living accommodation nearby, run by the same charity provider. Council A, where Joe is now ordinarily resident, is refusing to take over funding from Council B which had previously paid his out of county residential care fees. Some 14 months later, the social care provider (a medium sized charity) is owed nearly £50,000 from Council A for this one client. Members of the charity’s finance team chase Council A each week and include copies of previous correspondence and agreements. Council A continues to delay payments, giving the provider different reasons for not paying and passes the query around different council departments. The charity has continued to provide care and covered this gap in fees.”
While the powers-that-be seem unwilling to either acknowledge the scale of the problem or indeed have the confidence to untangle the mess, vulnerable people across the country remain in limbo, unable to move to the place of their choice because of bureaucratic wrangles.
As Anna McNaughton’s mother told me three years ago: “All Anna wants is to live in a suitable home – it’s a basic human need, not a luxury.” It’s a desperate situation that three years on, her words still have the same resonance.
Julie Heightley was so worried about her son Thomas suffering an epileptic fit at night that for two years she slept on a camp bed outside his room. The broken sleep and constant supervision of Thomas, who has autism and global developmental delay, was adversely affecting both Julie’s role as a carer and any prospect of independence for her son.
Now, thanks to a discrete network of wireless sensors dotted around the four-bedroom family home just outside Wolverhampton, Julie and Thomas, now five, are enjoying what Julie calls “a new lease of life”. Since the home was kitted out with the assistive technology two years ago, Thomas has been able to safely play and walk about the house independently without needing his mother’s 24-hours-a-day supervision. As well as having a slightly more hands-off approach to her five-year-old, Julie, a lone parent, has more time to spend her two older children who are in their teens.
Julie and Thomas with his older siblings
Assistive – or personalised – technology includes a wide-range of supportive but unobtrusive services and equipment, from personal alarms for elderly people, to seizure monitors and more sophisticated fingerprint recognition systems that allow you to open the door without keys. It can also include computer software, hand held devices or video call systems that increase social interaction and family contact.
As fans of such services and systems point out, the traditional view of this technology is that it involves a medical and prescriptive approach (see the comments on the related VODG blogpost), but the key issue is to bring it to the consumer market, widen its use among the general public and raise awareness about its potential.
As the publication stresses, the social care sector has embraced a huge amount of innovation in assistive technology, using new methods to complement the physical work of support staff. it is transforming lives for the better. But the use of such services, systems and equipment does not enjoy the higher profile of our counterparts in the health sector, despite the fact it is entirely in line with the “person-centred” approach that care providers are working towards and encourages choice, control and independence – social care watchwords.
Today’s report, with its real life stories of how technology is transforming the lives of vulnerable people, aims to change that: “Put simply, technology is part of our modern landscape. We use it for work, leisure, at home and on the move. It makes our lives easier. People with life-long disabilities or age related conditions should share that experience, benefitting from the advantages that tailor-made technological support can bring.”
Lol Butterfield, mental health campaignerI have lost too many friends and service users through suicide over the past 30 years.
We examine our consciences to see if we could have done more to prevent such deaths, that’s a normal human reaction. It’s what empathy and compassion is about. Being a nurse, as I am, is irrelevant, it is about being human. We consider those left behind to face the future and what support they need. It becomes a tragedy that spreads a pond like ripple of despair and pain. Nobody is immune from this rippling effect.
Often in our hour of need we turn to those who we know can provide support. Those who can help us to work our way through the grieving process. Sometimes just a listening ear or supportive approach by anyone is suffice. Sometimes more professional help is required. Everyone is different. We are all unique. We all deal with the inner pain following a death in the way we know best, our resilience levels dictate our strengths and coping abilities in times like these.
Recently, the All-Party Parliamentary Group (APPG) on suicide and self-harm prevention called for councils to develop and implement suicide prevention strategies. The APPG report revealed that more than a quarter (27%) of English authorities do not have any such specific strategy. As the APPG said: “The existence of any such plan is open to chance rather than determined by any national policy.”
The APPG wants councils to be obliged to develop a suicide prevention plan led by the director of public health or senior member of the public health team: “The plan should include provision for self-harm prevention and those bereaved by suicide.” As the group stressed, more than 5,500 people die by suicide each year in the UK and for people aged 15-24 it is the second largest cause of death after road accidents.
While I support anything that raises awareness of self-harm and suicide, I strongly feel that the responsibility for suicide prevention should not just be down to the passion of area ‘champions’ who have a particular interest in this. I believe all local authorities must seriously address suicide awareness, and prevention, as a matter of urgency. This is of particular relevance with increasing self-harm and suicide rates taking into account the recession and how this impacts on peoples lives at a personal level.
Mental health promotion is now under the control of local authorities, although personally I believe we all have a responsibility if working in social or health care to positively promote mental health.
As well as the personal costs to each family of a suicide the financial costs through lost earnings etc for a lifetime run into many thousands of pounds. As a compassionate and humane society I believe we have a moral duty to have in place coordinated strategic approaches to address the issue of suicide prevention involving all stakeholders. The NHS, local authority, the Police, The Samaritans, Cruse Bereavement counselling, community mental health support groups, and so on. In fact the list could be endless because in reality so many people are potential victims of suicide, directly or indirectly.
From a personal perspective, following my redundancy last summer my mood dipped. In fact it plummeted. Voluntary work at that time ensured my self esteem and confidence would stay above the water. I experienced ‘dark’ thoughts myself brought about by feelings of worthlessness and hopelessness finding myself unemployed after a lifetime of work.
The adjustment to the situation I now found myself in did not come easy. My intensive role in advising Zak Dingle in his depression storyline in the Soap Emmerdale conversely helped lift my own mood. I felt valued because I knew I was making a difference. I knew that I was raising awareness of mental illness to a large viewing public in a sensitive and non stereotypical way. Winning the Mind Media Awards a few months ago for this storyline further boosted my self-esteem even more.
Zak’s symptoms were intended to educate, encourage empathy, and promote more understanding of depression and how people can reach the point of suicidal ideation. They were intended to highlight how mental illness not only affects the person but also the loved ones of that person. I invested much time and effort to try to get this right and confess it wasn’t perfect, but nothing is. It helped me considerably as much as it helped others I had hoped to understand more and assume less about mental health.
I was also asked by a good friend to consider becoming more involved with Stamp Revisited, a wonderful, life changing for some, advocacy service on Teesside for those affected by mental illness. I had been a member for many years and applied to be on the group’s executive comittee. I was accepted.
This also boosted my self-confidence and esteem and played no small part in helping to lift my mood to a more acceptable level. Stamp Revisited is a charity and, as such, relies heavily on donations and the generosity of its volunteers. its aim is simple. To help those who struggle with mental ill health, any one of us at any time in our lives could be in this position. It would be fair to say their work has at times saved lives.
Knowing someone is there in your darkest hour can help to steer you away from the depths of despair. Specialist support can offer a more objective view on improving your personal situation that may have been lost in the spiral of depression. Insight can be lost in severe depression. Taking your own life can then become an option you would not have considered, ever. Knowing people are there to listen makes such a difference and words cannot explain how life saving this may be.




















 Daniel*, 21, describes how he was supported by the charity
Daniel*, 21, describes how he was supported by the charity  Karen McCulloch, Includem project worker, on how she supported Daniel:
Karen McCulloch, Includem project worker, on how she supported Daniel:



